Direct access colonoscopy means you can schedule a screening colonoscopy for yourself without needing to have a preprocedure visit with the doctor. This saves you time and money, and reduces the waiting time for your procedure.
Dr. Gandolfo explains how direct access colonoscopy is a convenient way to protect yourself from developing colon cancer in this short video!
Who is eligible for direct access booking?
You are age 45-75, have no concerning symptoms, and just need a routine screening colonoscopy.
You have a history of colon cancer in your family and your primary care provider told you to get checked.
You had a colonoscopy in the past that showed polyps and you are due for another routine colonoscopy now.
You took a Cologuard test or another stool test that was positive (abnormal) and now you need a colonoscopy.
Click the button below to schedule a colonoscopy. Even if you are not sure if you’re a good candidate for direct access, we will still reach out to you to figure out the best way to get you screened and help prevent you from developing colorectal cancer!
I made a video to help with the common problems that people encounter when preparing for a colonoscopy.
If you’re having trouble with the taste of the prep, nausea or vomiting from the prep, or the prep just isn’t working and you’re not clear, this video is for you!
In the US, colorectal cancer is currently the second leading cause of cancer deaths in men and women combined. Virtually all health professionals agree that screening average-risk people starting at age 45 for colorectal cancer is the best way to prevent this disease. There are a few highly effective tools available for colorectal cancer screening: This article will focus on the two most popular tests, colonoscopy and the Cologuard test.
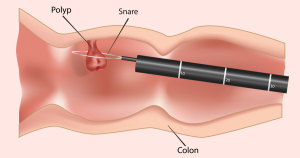
Most people are familiar with colonoscopy, but in case you’re not…colonoscopy is a safe 15-20 minute outpatient procedure that is done using sedation (so it’s painless) that entails using a flexible scope inserted in the rectum (the end part of the colon) and carefully advanced to the cecum (the other end of the colon) to inspect the entire colon lining for the presence of polyps, tumors, and other abnormalities. A polyp is a “precancerous” growth that is common and if not removed can slowly grow and eventually may turn into colon cancer. During a colonoscopy, the doctor can both find polyps and remove these polyps at the same time. Therefore colonoscopy can both diagnose cancer and polyps, but more importantly colonoscopy can prevent colorectal cancer from occurring in the first place by removing precancerous polyps years before they would have otherwise become cancer. A normal colonoscopy typically does not need to be repeated for 10 years. If polyps are found and removed, a colonoscopy will be recommended sooner, to make sure any new polyps that grow will be found and removed before having a chance to turn into colon cancer. Colonoscopy is considered the gold-standard colon cancer prevention test and is the preferred test by most medical societies.
Removing a precancerous polyp with colonoscopy.
Cologuard® is a non-invasive, commercially-available screening test for colorectal cancer. The test is ordered by a doctor (typically a primary care provider) and mailed to the patient’s house. When the urge to have a bowel movement strikes, the patient places the Cologuard collection device over the toilet and makes a deposit. There are a few simple preparation steps such as adding in a small amount of liquid that the company provides, and then the entire container of poop is mailed back to the company in the provided packaging. The Cologuard test looks for blood and certain DNA mutations in the stool to determine if a test is positive or negative. A week or so later the doctor gets a report indicating the result. If the test is negative, it only “protects” the patient for 3 years.
So which test is better, colonoscopy or Cologuard?
Well, it really depends on what the goals are…
As a general philosophy, it’s much more effective to prevent a disease from occurring rather than waiting for the disease to occur, then reacting to it. When the disease in question is colon cancer, preventing it starts with healthy diet and lifestyle as well as screening the population at large for polyps, the precancerous growths that cause colon cancer. To have a colonoscopy and remove a significant polyp is akin to stopping a future cancer from occurring in the first place. When effective preventive tests like colonoscopy exist, to wait until a patient has developed cancer and then treating the cancer is like waiting until you have been in a car accident to then put on your seatbelt…it’s too late. Although there are excellent treatments available for colorectal cancer nowadays, including surgery and chemotherapy, treating cancer is not the goal of screening. The goal of screening is to not develop cancer of the colon in the first place!
Typically, when an effective prevention technique exists (like removing precancerous polyps during colonoscopy) the earlier we can screen for colon cancer the better. This is why colonoscopy is the preferred test for younger healthier people starting at age 45. Save a 45-50 year old from colon cancer and you will potentially give that person 30-40+ years of life having not developed colon cancer. Saving a 79 year old from colon cancer is still a commendable goal, however the average 79 year old typically won’t have as many quality years left “in the tank” compared to the average 45 year old.
So why does this philosophical stuff matter when it comes to picking a colorectal screening test? Well, understanding what these tests do helps you understand how to apply the proper test to your individual goal.
If this article is already too long and you just want the bottom line, here it is: Colonoscopy is the superior test for most people, especially “younger” people (age 45-mid 70s). It can both detect and (more importantly) prevent colorectal cancer. It is semi-invasive and less convenient when compared to Cologuard testing. Cologuard is an easier test but plagued by false negatives and false positives. Cologuard does not necessarily prevent cancer, it only detects cancer after cancer has occurred, or at best detects large polyps that are close to becoming cancer. Cologuard should be considered for older patients (age 75+), for patients that may not have the best overall health, or for patients who have specific reasons why they cannot have a colonoscopy.
OK, you asked for it! Here are more details, starting with the Cologuard test:
The study that determined the characteristics of the Cologuard test basically performed the test on almost 10,000 patients at average-risk of colon cancer, and then had the patients undergo colonoscopy as the gold-standard test. The results of the Cologuard test were not available to the patients or the endoscopist at the time of the colonoscopy. The major results of this study showed that the Cologuard test had a sensitivity (the amount of times it picked up colorectal cancer when cancer was indeed present) of 92%. It was far less sensitive for picking up advanced precancerous polyps, at only 42%. It turns out that sensitivity is the main thing we care about in a screening test: we want the test to miss none of the patients who have the disease. A perfect screening test would have a sensitivity of 100%, meaning that if 100 people have colon cancer and have the test, all 100 people will get a “positive” test result, meaning no false negative tests.
Sensitivity isn’t everything however…we also want a test that gives a negative result when someone does not have the disease in question. That is, if you take a group of 100 people that do not have colorectal cancer, a perfectly specific test will have 100 “negative” results, meaning no false positive tests.
What does a positive Cologuard test mean?
First and foremost, a positive result on the Cologuard test means that you need to have a colonoscopy. Not a virtual colonoscopy, or another stool test, or another scan of some sort…you need a real optical colonoscopy. Luckily, only about 4% of people with a positive Cologuard test will have cancer found on colonoscopy. 51% will have a precancerous polyp. The rest (45%) will have nothing found on colonoscopy. So to simplify even further, just a little more than half of people with positive results will have something abnormal (cancer or a polyp) found on colonoscopy.
What does a negative Cologuard test mean?
A negative test means that there is a less than one-percent chance of having cancer found on colonoscopy. However, about 34% of people with negative tests still have precancerous polyps found on colonoscopy, with the remainder (66%) of people with negative Cologuard results having truly negative colonoscopies.
What is immediately apparent from these numbers is that Cologuard rarely misses cancer. However, if we count polyps as a significant finding, there are plenty of false-positive results (45%) and plenty of false-negatives too (34%).
A word on how health insurance companies view Cologuard…
While not important to the medical reasoning behind choosing colonoscopy or Cologuard, for some people it is important to note the finances of each test. Either colonoscopy or Cologuard can be considered a screening test, and is typically covered by health insurance plans without an out-of-pocket cost. However, if a Cologuard test is positive (remember that 45% false positive rate discussed above), the insurance company now views the necessary colonoscopy as a diagnostic colonoscopy, not a screening colonoscopy. Diagnostic tests often have an out-of-pocket responsibility for the patient and in the case of a colonoscopy this can be in the thousands of dollars range. This is something rarely discussed when ordering a Cologuard test in the primary care setting, but that we often need to educate patients about when it’s time to book their colonoscopy to follow up a positive Cologuard test.
What about colonoscopy? Are there any downsides?
In good hands, colonoscopy is an excellent test—it’s the best test we have in the fight against colon cancer. However, no test is perfect and colonoscopy is no exception. Even though colonoscopy is the gold-standard test, here are some of the negative things to know about colonoscopy.
Colonoscopy requires a bowel preparation, meaning you have to take either a liquid prep or pill prep to clean out the colon the day before. It’s not painful, but prepping for a colonoscopy is far from a good time. Colonoscopy has small but real risks, such as bleeding, infection, perforation of the bowel, and anesthesia problems. However these risks are very rare, and in with a skilled team the risk of a serious complication is far less than 1 in 1,000 procedures. Colonoscopy also has a miss rate for polyps and even cancer. It is very hard to define an actual number of missed lesions because it’s difficult to perform a study on the gold-standard test (colonoscopy) as there is no better test to compare it to. That being said, colonoscopy can miss small polyps around 20% of the time, and can even miss cancer a few percent of the time. The devil is in the details however: Missing a significant lesion during an outpatient screening colonoscopy in a properly prepped patient (meaning the patient did the bowel cleanse effectively) with a doctor that performs high-quality colonoscopy (meaning the doctor spends adequate time and uses excellent technique to find and remove polyps) is quite a rare event and is something that is difficult to study given variations in quality practice between doctors even in the same community or hospital system.
Here is a quick pros and cons table to help clarify all of the above
Measure
Colonoscopy
Cologuard®
Prevention of colon cancer?
Yes
Not really
Repeat a normal test every
10 years
3 years
Overall convenience
Bowel prep and 1 day off work
No prep but have to handle stool
Overall invasiveness
Moderately invasive
Not invasive
Accuracy
Very accurate
Not very accurate
Biggest upside of the test
Better cancer prevention and accuracy
Easy and can do it at home
Biggest downside of the test
Bowel prep and less than 0.1% chance of complications
Lots of false positives that will require a colonoscopy anyway
How do I choose between colonoscopy and Cologuard in my practice?
I typically reserve Cologuard testing for patients that just need to know if they have cancer right now, and are not in good condition to undergo colonoscopy due to other major health issues. A patient that has not been screened recently who is approaching 80 years old, and who has one or more major cardiovascular or pulmonary issues is a good candidate for Cologuard testing. For pretty much everyone else, colonoscopy is by far the better test.
References:
Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med 2014;370:1287-97.
The colonoscopy prep experience is by far the worst part of the whole procedure. For years, patients have been asking “Isn’t there a better way to do the prep?”
Well, now there is! There is a prescription bowel prep called Sutab that I have been using for the past two years for most of my colonoscopy patients. Sutab comes in a kit which includes 24 pills and a container to measure the water, and it couldn’t be any easier to take. Most of my patients that have used the older liquid preps in the past are pleasantly surprised after using Sutab for the first time!
Here is a short video I made showing you how to use Sutab. I also cover the diet you should follow to make sure your “clean out” is as clean as possible, and how to handle the common side effect of all bowel preps…nausea.
In this video, Dr. Gandolfo will show you what NOT to do if you want to have an easier colonoscopy prep experience. He will also share five tips to help you handle the pre-colonoscopy clean-out like a champ!
If you want more information about colonoscopy, be sure to download our free ebook today! It will answer any question you can think of about colonoscopy, even questions you didn’t know you had!
Click the picture of the book below to get it delivered to your inbox!
March is Colorectal Cancer Awareness Month, but this video holds true all year!
Dr. Gandolfo will review the basics about colon cancer here: What it is, how to prevent it with diet and lifestyle, and how to get screened for this common and deadly disease.
If you’ve got questions about colonoscopy, this is the book you need to read!
Everything You Need To Know Before Your First Colonoscopy is packed with everything you could ever want to know about having a colonoscopy! I will take you step-by-step through the procedure, and answer all of the common questions that I usually get from patients about the test.
Here is the table of contents from the book:
Want a copy of the ebook delivered right now? Enter your email address below, then go check your inbox. Once you click the link to confirm your email address, you will receive the book by email immediately!
Your email will never be shared or sold. It will be used to occasionally send you new articles as I publish them on my informational blog Retroflexions.
Bowel prep, or that stuff you need to drink to get cleaned out for your colonoscopy, is never something that one looks forward to doing. You knew that drinking the prep was a necessary evil to ensure a high-quality colonoscopy, but what do you do if you followed all the instructions but the prep simply didn’t work?
If you’re reading this while in the midst of a potentially failed bowel prep don’t despair! There are many ways to salvage a bowel prep and still have a safe, high-quality colonoscopy the next day. It all depends on what time you take action; If you wait until 2 hours before the procedure is scheduled than yes, it’s probably too late to do much. However, if you’re already having issues the night before you can totally recover from this and be fine. This is what I usually recommend, based on the issue at hand:
“I drank the first dose of the prep and nothing happened.” I usually tell patients to wait several hours before panicking. If you have waited 6 hours and there is no bowel activity whatsoever then at that point I would recommend taking either 10 mg of bisacodyl by mouth, or giving yourself an enema. If you’ve done all that and still nothing happens, then it’s probably time to call your doctor and ask for suggestions.
“I drank the first dose of the prep but vomited most of it up.” Unfortunately, you will need more prep then. This usually requires a phone call to the doctor explaining the issue and often an alternative prep is recommended. In selected patients, I would usually recommend Miralax prep or using magnesium citrate instead–both of which can be purchased over the counter.
“I can’t drink the first dose of the prep because it tastes horrible! Yuck!” Try putting the prep in the refrigerator and making it as cold as you can tolerate. Much of the taste disappears when you really chill the prep. You can also call your doctor to see if an alternative prep is an option for you. Ultimately this is also a case of mind-over-matter…it’s unpleasant but sometimes you just have to do it anyway!
“I drank both doses of the prep and my bowels are still not clear” This is a common issues with some bowel preps. It really depends on what time this happens. If you did all the prep the night before, then there is plenty of time to follow the prep with a bottle of magnesium citrate and a large volume of clear liquids. If you notice that you are not clear the morning of the procedure, you can still drink magnesium citrate but really need to finish drinking it about 4-5 hours before the procedure is scheduled to start. This gives it enough time to have an effect, and also keeps you well within the 2 hours safety window for ingestion of clear liquids with respect to receiving anesthesia. However, if the procedure time is close (2-3 hours away) and you’re still not clear, then the only real option is to give yourself an enema or two. You can always reschedule the procedure if you have to, but realize that you already completed the bowel prep and will therefore have to do the entire prep again if you need to reschedule!
On May 30, 2018, the American Cancer Society (ACS) released new guidelines regarding colorectal cancer screening for the average-risk individual. The big news is that they now recommend that screening for colorectal cancer begin at age 45 rather than age 50. This reduction in the starting age was in reaction to recent data showing that colon cancer is increasing in younger Americans for unclear reasons. By screening people at a younger age, the hope is that we can detect and prevent colon cancer in more people.
The ACS states that 20% of new cases of colorectal cancer occur in the younger-than-55 crowd. Furthermore, despite a general downward trend in colorectal cancer in the over-50 population, the risk is actually rising slightly in the subgroup of people aged 50-54. These are the cases of cancer the new guidelines are trying to prevent. The ACS is pragmatic in acknowledging that people don’t typically sign up for a colonoscopy exactly on their fiftieth birthday…in fact many wait a few years or more after age 50 to get screened. By pushing the starting age up by 5 years there will likely be a benefit to these patients who would otherwise be late to the colonoscopy party.
The consequences of these recommendations are potentially huge. If these guidelines are followed, an estimated twenty million additional people are now eligible for colon cancer screening. However, the ACS does not specify any one best choice for colorectal cancer screening and states that colonoscopy, stool DNA testing (Cologuard), virtual colonoscopy, and stool testing for occult blood with Guaiac-based tests or FIT testing are all equivalent. I think that by now we know that all tests are not really equivalent, with colonoscopy being the gold-standard test, but with millions of people not getting any type of screening at all, any test is better than nothing.
“My thirties are going great! And in a few short years, I’ll need my first colonoscopy!”
A few caveats about these new recommendations:
The ACS states that the recommendation to start screening at age 45 is a qualified recommendation, meaning that there are clear benefits of screening at this younger age but there is less certainty about the exact risk-to-benefit ratio of the recommendation. This is opposed to a strong recommendation, which means the benefit is clear and almost everyone should do it. (Beginning screening at age 50 remains a strong recommendation from the ACS.)
Other guideline-producing organizations such as the US Preventive Services Task Force (USPSTF) have not changed their recommendations for colorectal screening, which still remain at age 50 to start.
Just because the American Cancer Society changed the recommendation to age 45, doesn’t mean that insurance companies are going to cover the testing! This is perhaps the most interesting part of these new guidelines…who is going to pay for this?
Starting screening earlier is definitely going to pick up and prevent more cancers than starting later, however is 45 the best age to start? Surely starting at 44 would pick up even more cancers! I bet starting at 40 would pick up even more than that! What I’m trying to illustrate is how there can be a slippery-slope with these type of recommendations: You will always find more cases of colorectal cancer if you start looking for it in younger and younger people. At what point do the risks of screening more and more people start to outweigh the benefits? Only time and more research will help answer this question.
What about the truly early-onset colorectal cancer patients? These are patients diagnosed in their twenties and thirties…how do we detect them before they develop the disease? I doubt anyone will recommend starting routine screening colonoscopies at age 18! This very young onset colorectal cancer may just behave differently than the typical sporadic colon cancer that develops later in life. We need to develop different ways of finding the young patients at risk, and determine why the risk is rising in the younger population.